CASE 5: Revision for implant wear of the polyethylene liner with very high blood titanium levels

The Story
“Camila first attended my clinic at the age of 71, with pain in her right hip. This was causing her mobility issues and starting to impact her daily living: she was unable to walk for more than 5-minutes, and putting on shoes caused her significant discomfort.
She was operated on 12 years prior receiving a Corail Pinnacle right total hip replacement. Unfortunately, the femoral stem was proud, which created a leg length discrepancy with a long right leg.”
The Investigation
On clinical examination Camila was mobilising with the aid of a walking stick. She was able to flex the right hip to 90 degrees. There was significant stiffness in the joint, and her pain was exacerbated by internal and external rotation of the joint. She walked with a Trendelenburg gait and was Trendelenburg positive on the right side. There were no signs of infection.
Her Oxford Hip Score for the right hip was 17/48.
Her blood inflammatory markers (CRP and ESR) were normal helping to rule out infection.
Her cobalt and chromium levels were normal.
She had an elevated titanium level at 364ppb.
The Evidence

Anteroposterior plain radiograph demonstrating a cracked right polyethylene liner within a titanium shell. The head is bearing onto the titanium shell.
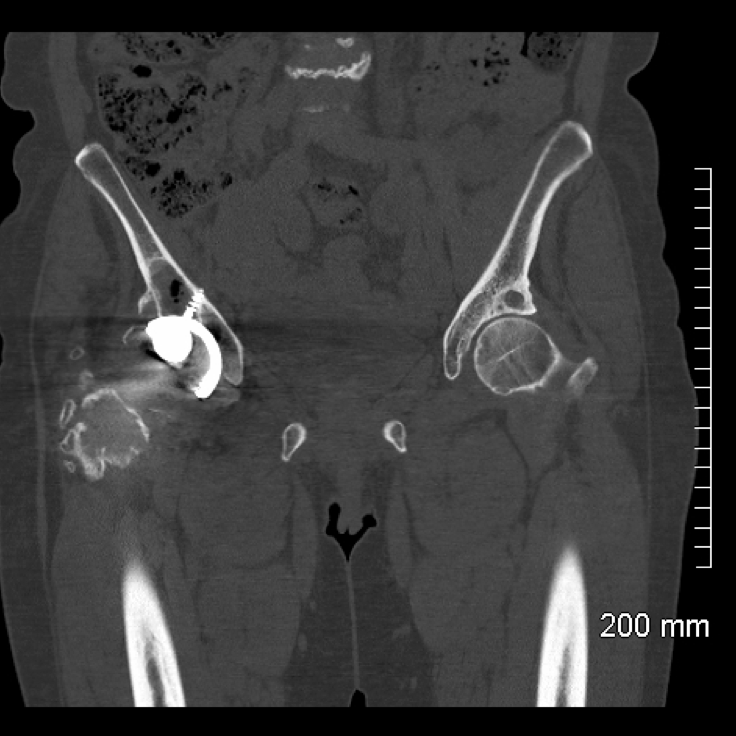
Coronal CT demonstrates evidence of acetabular loosening with a periprosthetic lucency surrounding the superior acetabulum. Osteolysis is seen over the greater trochanter with fragmentation and surrounding heterotopic ossification (calcification of the surrounding soft tissue). Degenerative changes are seen in the left hip with subchondral cysts and a cortical breach. There is also some lumbrosacral degeneration.
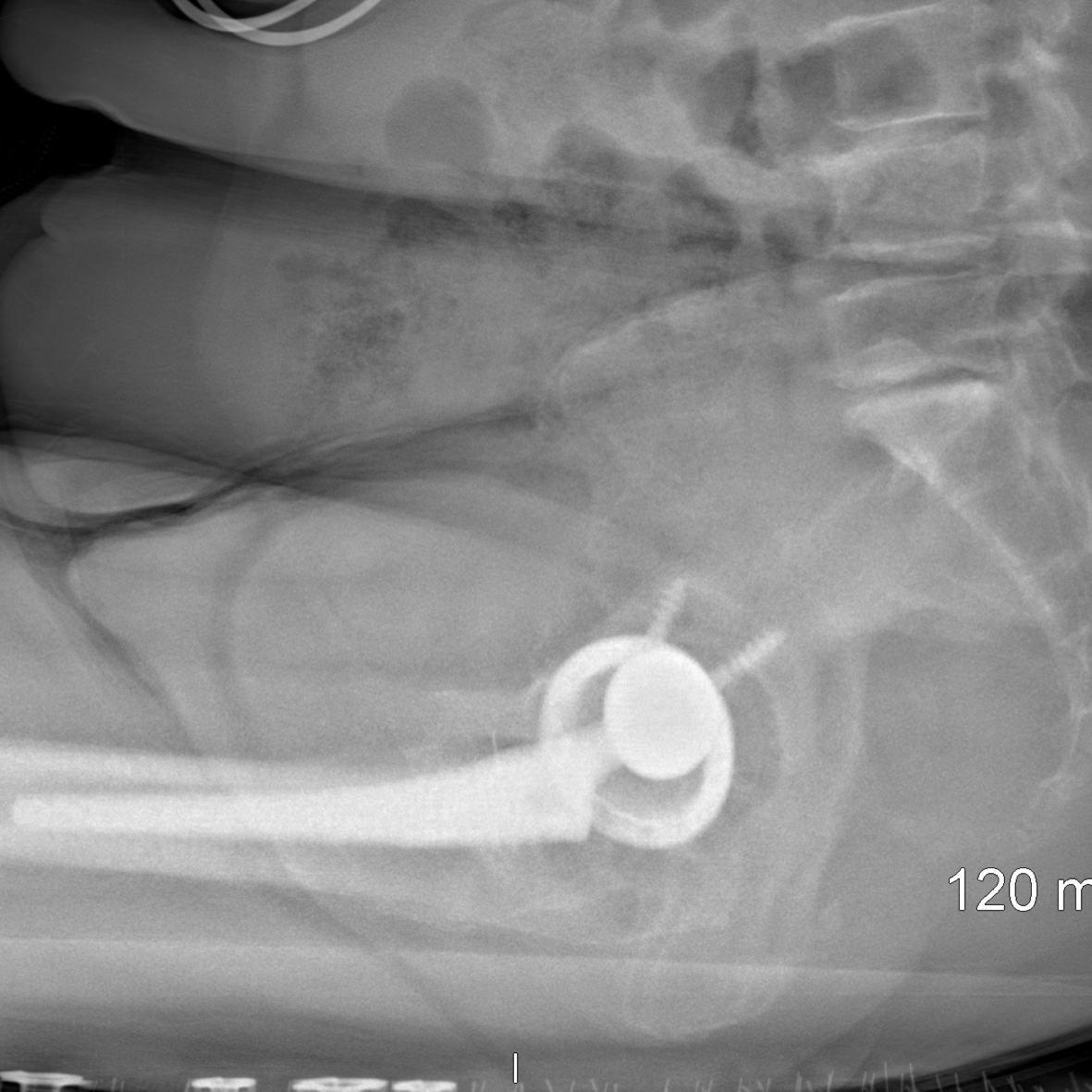
EOS scan showing the articulation of the femoral head within the titanium shell when Camila is sitting.

Coronal MRI demonstrates the femoral head articulating with the titanium cup. The MRI shows a small joint effusion with good surrounding musculature. Bony erosion of both the anterior and posterior columns of the pelvis and the anterior portion of the greater trochanter is seen on the right side.
The Diagnosis
Camila was diagnosed with a failed right total hip replacement with extensive wear of the polyethylene liner. The cobalt chromium femoral head was articulating on the titanium acetabular shell.
The Plan
A plan was made to revise her right total hip replacement using a jumbo acetabular cup due to the erosion of both the anterior and posterior columns. We planned to replace the femoral stem to correct her leg length discrepancy.
The Operation
Camila underwent a right total hip replacement using a posterior approach. After careful dissection, samples were taken and sent for microbiology and histology. The cobalt chromium head was removed and the femoral stem explanted with MIDAS Rex pencil reamers, flexible osteotomes and a Symmetry extractor. We were careful to maintain as much bone stock as possible.
On the acetabular side, there was extensive metallosis with a ‘black pelvis’ which required debridement. The acetabular cup was explanted with minimal bone loss and the broken screws were removed. The acetabulum was reamed to 63mm using serial reamers. This was then extensively washed with NaCl and Savlon. We reverse reamed bone graft into the acetabulum, and implanted a 64mm shell which was further secured with multiple screws achieving good fixation.
The femur was then prepared and a Restoration stem was implanted. We performed a trial reduction and the joint was stable with a good ROM and equal leg length. The definitive polyethylene liner and ceramic femoral head were implanted and the surgical site was washed and closed.
The Outcome

Anteroposterior plain radiograph of the pelvis demonstrating the bilateral revision with acetabular bone graft on the right hand side.

Lateral plain radiographs of the pelvis demonstrating the jumbo acetabular cup in situ with a long Restoration stem.
The Verdict
“The Mayo definition of a jumbo cup is a diameter >62mm for females and >66mm for males. These cups were the ‘workhorse of revision hip surgery’ — but they risk removing anterior and posterior bony columns. In this case, the acetabular bone was black and poisoned by the titanium and so had to be removed back to viable bone.”
-
We know that high blood titanium levels can signify an implant problem:
However, we do not know the clinical significance of titanium released from implants. Information on the blood levels of titanium from well functioning hip implants is now available:
-
-
Besides polyethylene liner damage as a cause of high blood titanium levels, ceramic liner fracture is another cause, as shown in this case:
Acetabular Reconstruction - Step One - Case Two