CASE 28: Revision of a loose cup using an anti-protrusio cage

The Story
“Nala was unable to walk and struggling with severe night time pain in her left hip when she first came to see me. Her past orthopaedic history was not uncommon, with previous bilateral metal on plastic hip replacements which had lasted for about 20-years; followed by a revision of the left hip secondary to osteolysis 3-years prior to us meeting.
She was having to take NSAIDs to try and stem the pain but unfortunately this was neither fully effective or sustainable. We started an extensive investigation to understand the cause of her pain.”
The Investigation
Clinical examination demonstrated a very painful and stiff left hip. She had extreme difficulty straight leg raising on the left hand side and was only able to walk a few steps across my clinic room. She had previously been told that her left hip would not be reconstructable, so Nala thought this was the best her walking could be.
To rule out infection we performed a normal set of blood inflammatory markers, none of which were raised.
The Evidence
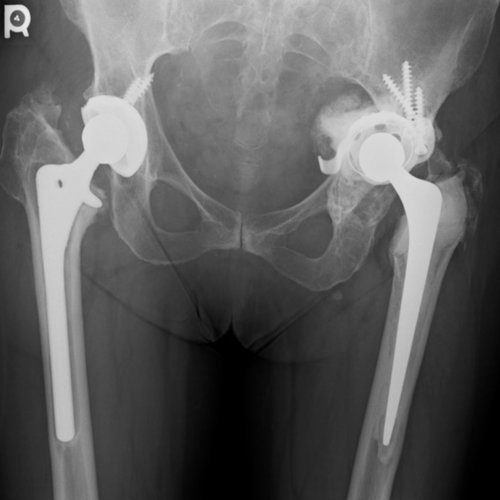
Anteroposterior (AP) radiograph of both hips showing bilateral hip replacements with polyethylene liners (it is difficult to distinguish ceramic from metal heads). The right hip stem is radiographically loose with radiolucent lines in all 7 Gruen zones.

Lateral plain radiograph of the left hip. The acetabular cage is loose and it is protruding into the pelvis. The stem on the left hand side is well fixed after her revision procedure.

Coronal CT demonstrated an intact posterior column on the left side.
The Diagnosis
Nala was diagnosed with loosening of the right stem and migration of the left acetabular component. She was offered revision of both sides, starting with the left as this was causing her more discomfort.
The Plan
We planned to retain the well fixed left sided femoral stem but remove all of the acetabular components. Our plan was to use an anti-protrusio cage (like the one below) to form a rigid base in which we could cement a new acetabular liner. Nala had very little bone stock remaining, so with the technology at the time, this was the best option to try and reconstruct her left hip joint.

Anti-protrusio cage - This image shows a left-sided cage. The inferior, spiked flanged is designed to be impacted into the ischium or lie on its outer surface. The superior flanges are designed to fix into ilium.
The cages come in a range of sizes. The flanges are difficult to shape to the bone and there is a no fixation into the pubis. A polyethylene cup or dual mobility metal liner is cemented into the cage.
The Operation
A posterior approach to the hip was used protecting the sciatic nerve.
The cage that she had in was loose, so it was removed with all the acetabular metal work and the polyethylene liner.
A new cage was inserted and then a new polyethylene liner was cemented into the cage.
The stem was retained.
Leg length and stability were both good.
The Outcome

Anteroposterior plain radiograph of the pelvis post-revision. This demonstrates a left-sided anti-protrusio cage surrounded with bone graft and a cemented polyethylene cup . The stem was retained as this was well fixed.

Anteroposterior plain radiograph of the pelvis taken three years after the left hip reconstruction. There has been no migration of the cup-cage construct. Note that the right side has been revised.
Nala was very happy with the outcome of her left sided hip revision. After a revision to the right hip, Nala was able to walk several miles and was no longer requiring analgesics. We were both very happy with the outcome of her anti-protrusio cage.
The Verdict
“It was difficult to know if there was pelvic discontinuity prior to starting the operation (despite CT scanning) but the presence of a failed small cage requires preparation for a larger reconstruction. An alternative would have been to use a cup-cage construct and less bone grafting.
Nevertheless, the bone graft incorporated and the anti-protrusio cage remained well fixed up until last follow up at 5 years post operative.
There are newer technologies available to make the operation easier for the surgeon and patient.”
-
There are modified designs of the original anti-protrusio cage. Originally it was designed for the ischial flange to be embedded within the ischium and then screwed onto the surface of the ilium in case of pelvic discontinuity.
The diagnosis of pelvic discontinuity is difficult and usually requires CT.
Modifications have allowed it to be screwed onto the surface of the ischium.
The most successful results are when it is combined with a cup: a large uncemented cup fills the defect and is protected by a cage overlying the cup; a polyethylene liner is then cemented into the cage.
-
-
Please see the custom acetabular reconstruction cases for comparison:
Acetabular Reconstruction - New Technology - CT Planning 3D Printing - Case One