CASE 9: Primary hip replacement with a massive acetabular defect from trauma, using a custom 3D-printed cup

The Story
“After almost four decades, the effects of a life-threatening pelvic fracture were becoming increasingly difficult for Sadiq. His fracture had resulted in other injuries, including damage to his lumbar spine nerve roots and his other hip. The pain was affecting Sadiq’s mobility and his ability to cycle and play tennis.
After one year of clinical and imaging assessment we decided to go ahead with a 3D-printed custom implant to reconstruct his hip. Due to the anatomy of his left hip being complex, with a posterior facing socket, I knew this was going to be a reconstruction challenge.”
The Investigation
Sadiq presented with pain in his native left hip at the age of 55. 36 years previously he had a conservatively managed left acetabular fracture with damage to the sciatic nerve.
He also had an asymptomatic right hip resurfacing, done for osteoarthritis.
On examination:
Sadiq was mobile with the use of a stick.
He had significant leg length discrepancy and a left shoe raise was in place.
Trendelenburg gait was observed.
His left leg was stiff.
He was able to straight leg raise on the left side but had little abduction or rotation of the joint.
No abnormalities were detected in the right hip joint.
He had reduced sensation in dermatomes L4, L5 and S1 on the left side in keeping with his sciatic nerve injury.
A scar was noted on the left lower leg associated with previous tendon transfer surgery to correct a foot drop.
The Evidence


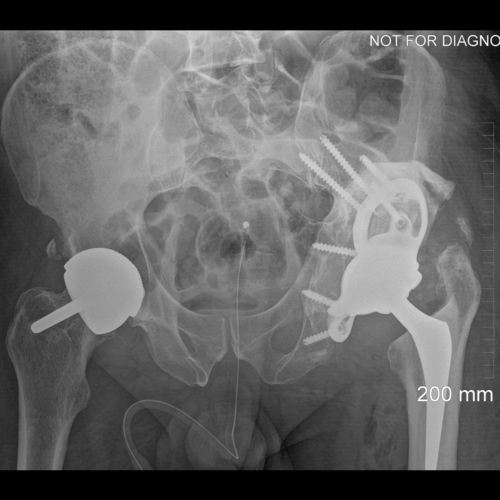
Anteroposterior and lateral plain radiographs showing left hip osteoarthritis secondary to acetabular fracture and a right femoral Birmingham metal-on-metal hip resurfacing.
The Diagnosis
Sadiq had severe osteoarthritis of the left hip with very disrupted anatomy due to previous acetabular fracture. There was good acetabular bone stock and a high centre of rotation. The right hip resurfacing had a loose femoral component, which had fixed in a stable position.
The Plan
We decided on a custom CT planned ProMade implant – 3D printed with trabecular titanium.




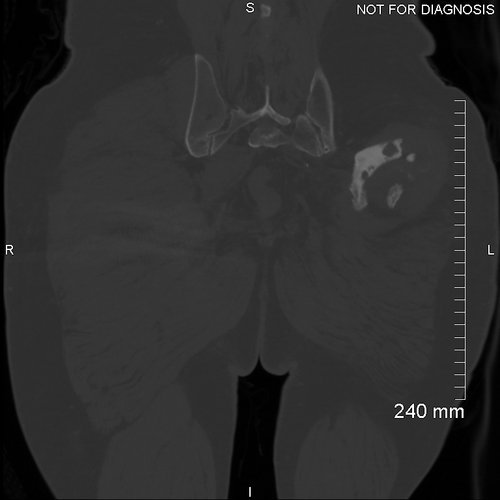












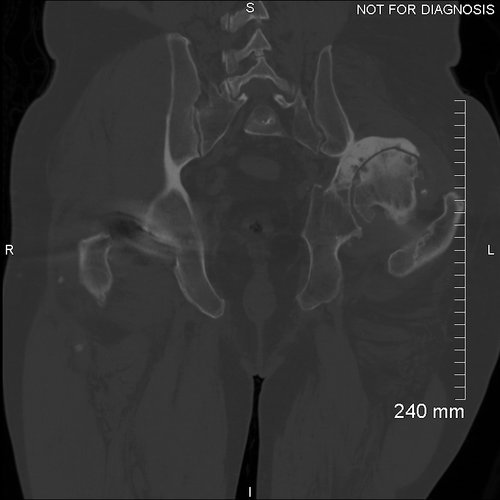
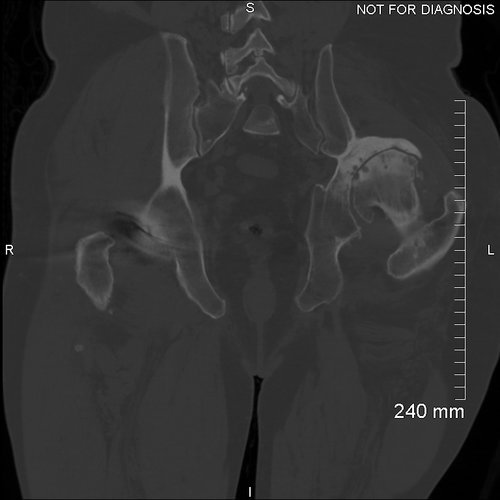
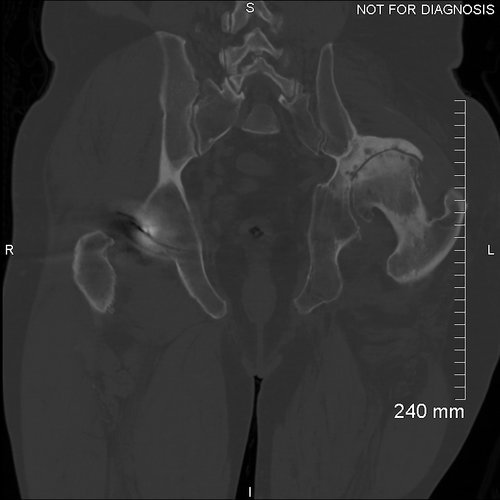
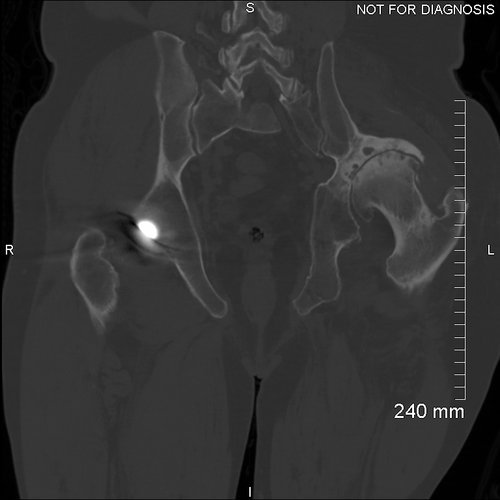






















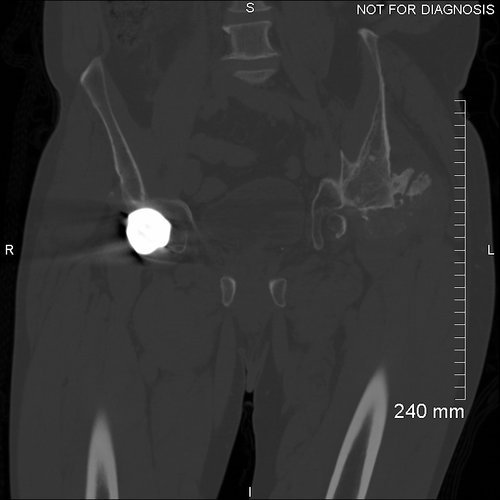

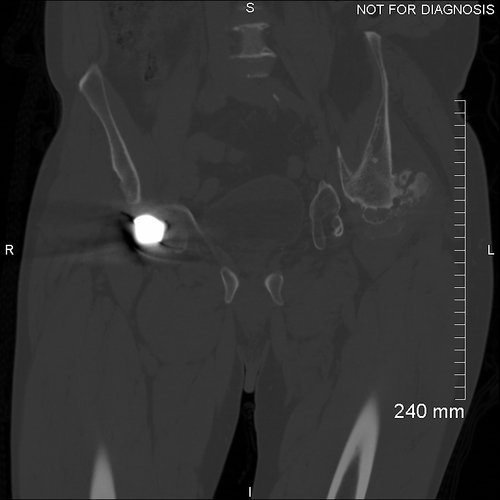

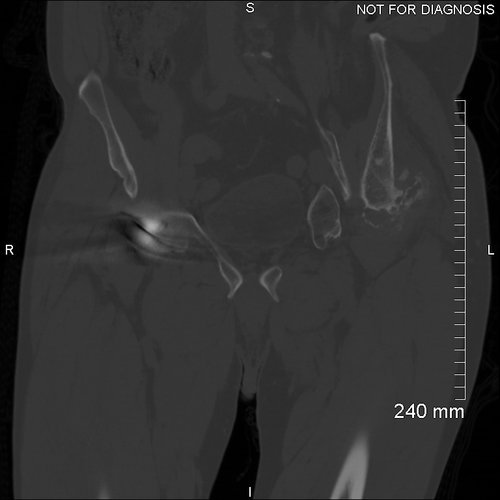


Coronal CT - showing a significantly abnormal left acetabulum with postero-superior dislocation of the left femoral head leading the neo-acetabular formation at the posterior of the left iliac blade. The neo-acetabulum is retroverted by 22 degrees. This was used to design the custom acetabular implant.
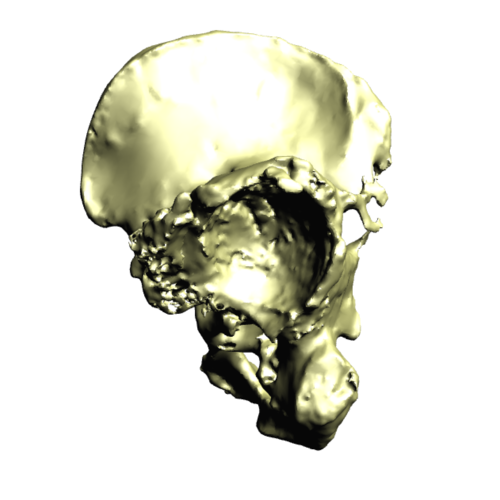
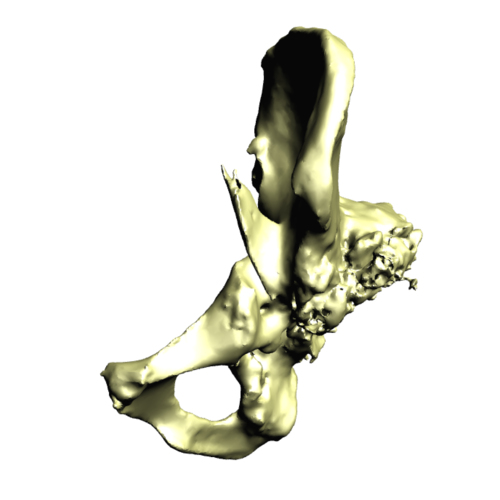
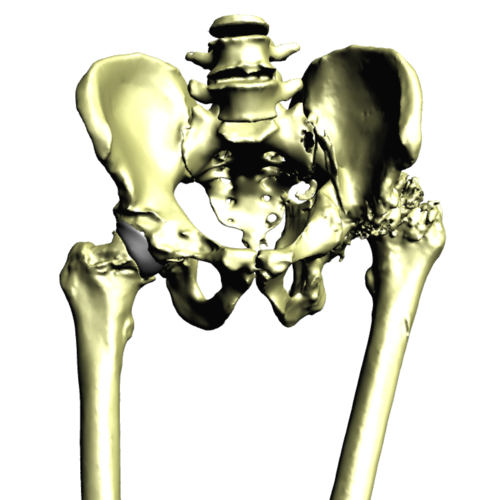
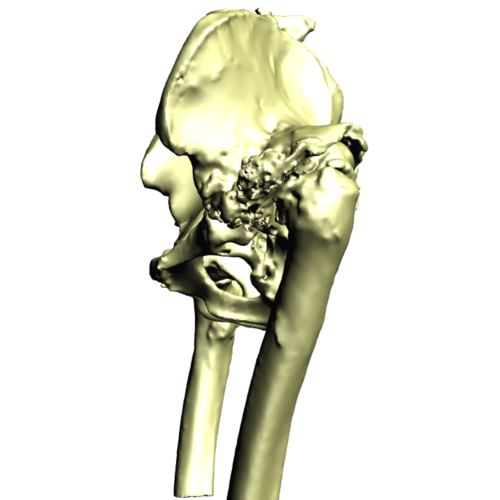
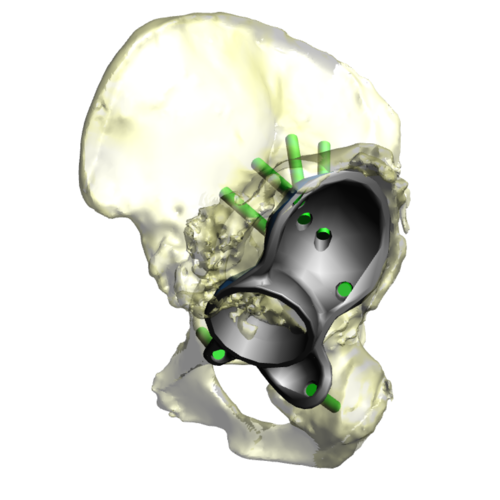
3D CT reconstruction showing the hemipelvic defect.
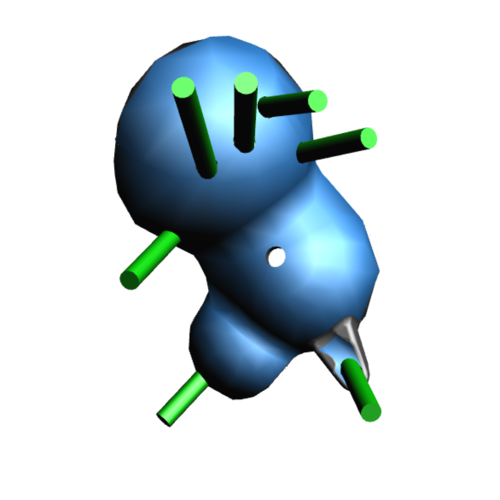
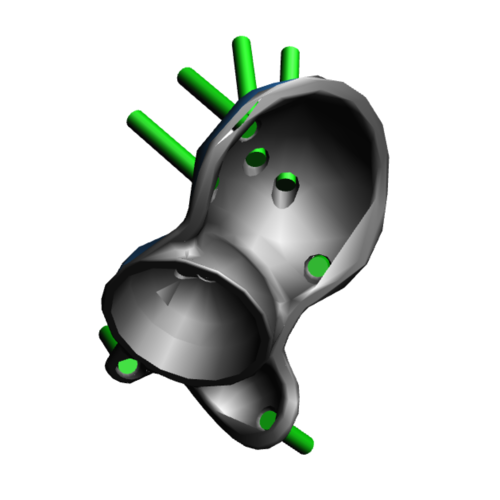
Implant design showing the custom acetabular implant designed around this patients bony anatomy. The blue areas highlight regions of trabecular titanium.
The Operation
We used an extensive posterior approach to the hip and used a nerve stimulator to find the sciatic nerve within the scar tissue. Patient specific instrumentation (PSI) guides were used for the bony preparation of the acetabulum. These guided three areas of reaming of the acetabular bone.
The custom acetabular implant was then secured with all screws as planned and a dual mobility liner was used. We used a cemented femoral C-stem with a ceramic head. Stability and leg length were assessed as were the nerves which were well functioning.
We washed the surgical site with Savlon and normal saline, before closing it with Vicryl, Monocryl and glue.
The Outcome
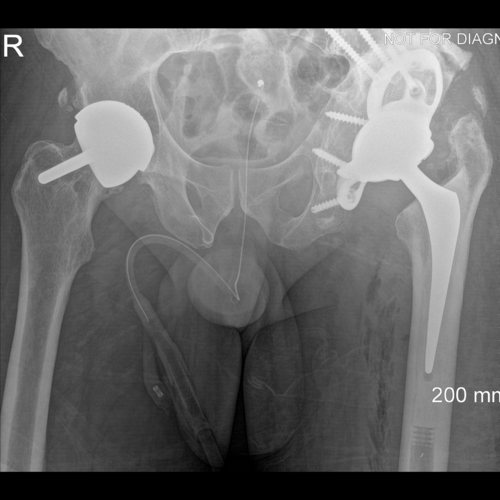
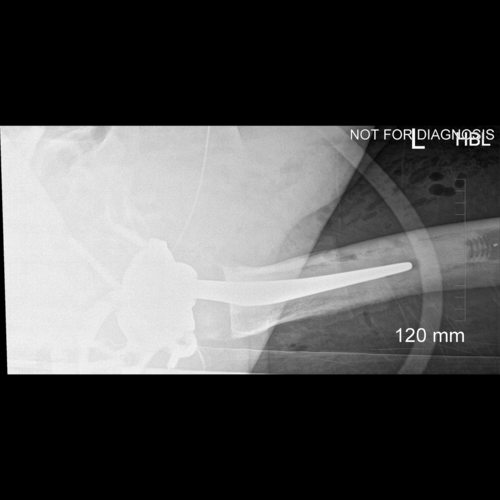
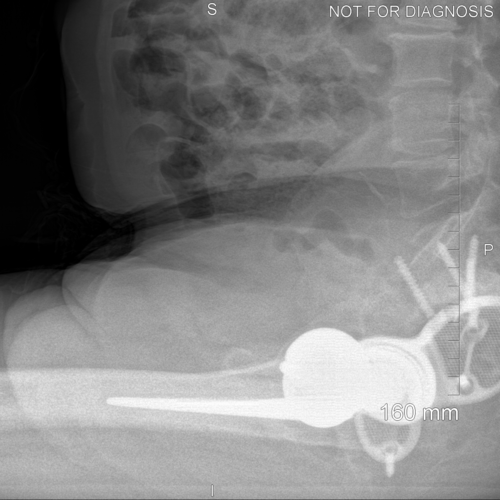
Anteroposterior and lateral plain radiographs taken after the operation showing a well positioned 3D-printed acetabular component and cemented femoral stem.

EOS scanning (low radiation dose, 3D scanning in functional positions of standing and sitting) taken after the operation.


Anteroposterior and lateral plain radiographs taken 6-months after Sadiq’s operation.
Nine weeks after the operation, Sadiq was recovering well and his wound was showing satisfactory healing. He was walking with two crutches and was able to straight leg raise. He was very happy with the correction of his leg length discrepancy. A plan was made to wean off the crutches, continue to rehabilitate with an exercise bike and Pilates and review in six months’ time.
The Verdict
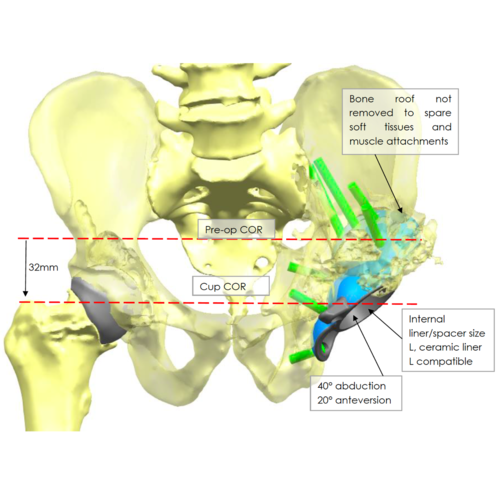
“The anatomy of the acetabulum was severely distorted by Sadiq’s previous acetabular fracture. The main volume of bone was posterior but placing the new socket here would have risked dislocation, early fatigue of the implant and increased wear of the bearing surfaces. We managed to recreate a near-normal centre of rotation of his hip despite the severely distorted pelvis.
This is a primary implant and it took more than 12 months for the patient and I to be confident that surgery was the correct decision. Neither of us has any regrets; Sadiq is very happy with the results.”